

Weight-Loss Peptides in 2026: What the Trials Actually Show, and Who Stands Between You and the Syringe
Written by Hana Costa, staff writer. Last reviewed March 2026.
There are, broadly, two ways to be wrong about weight-loss peptides. One is to assume they’re all snake oil because a few of them are. The other is to assume they’re all as well-tested as the famous ones, because the marketing borrows the same vocabulary. Both mistakes come from treating “peptide” as a single category, when it isn’t one. A peptide is simply a short chain of amino acids. That description covers semaglutide, which has been studied in tens of thousands of people, and it also covers a compound whose only real evidence comes from mice. The word tells you almost nothing about how much you should trust the claim attached to it.
This piece tries to hold two separate questions apart, because most articles on this topic quietly merge them. The first question is scientific: does the compound have real human evidence that it causes weight loss? The second is practical: even for the compounds that do, how do you actually obtain one safely, and who is checking that it’s appropriate for you? Getting the first question right and ignoring the second is how a person ends up self-administering a medication with a boxed warning [9] based on a vial that arrived with no clinician involved anywhere in the transaction. This page works through the evidence compound by compound, then works through the providers people are actually choosing between.
A note on sourcing before any of that: every figure below traces back to a trial, an FDA record, or a peer-reviewed paper, all listed at the end. Readers are encouraged to check them rather than take this article’s word for anything.
Why the evidence and the marketing point in different directions
Search “peptides for weight loss” and the results tend to flatten everything into one list: semaglutide beside AOD-9604 beside MOTS-c beside 5-Amino-1MQ, as though they belong to the same tier of evidence because they belong to the same search query. They don’t. Some of these are FDA-approved active ingredients with large randomized trials behind them. One is investigational, meaning it has strong trial data but hasn’t finished the approval process. Others have never been tested in a human weight-loss trial at all, only in mice or in observational studies of something the body already makes.
The confusion is not accidental. The GLP-1 medicines earned their reputation the hard way, through years of trials involving thousands of participants. Everything else in the “fat-loss peptide” category gets marketed alongside them, inheriting some of that credibility without having done any of that work. A fair reading of the evidence tends to run backwards from the marketing volume: the loudest claims usually sit on the thinnest data.
The evidence, compound by compound
Semaglutide: the validated original
Semaglutide is a GLP-1 receptor agonist, and it is the compound most people mean, whether or not they realize it, when they say “weight-loss peptide.” It works by engaging the GLP-1 receptor, which slows gastric emptying, blunts appetite, and improves glucose handling [8]. Its trial record is large and mature. It is also, worth remembering, a prescription drug with real cautions attached: the approved labeling carries a boxed warning for thyroid C-cell tumors and lists a personal or family history of medullary thyroid carcinoma or MEN 2 as a contraindication [9]. That is precisely the sort of history a prescriber is trained to screen for and a research-chemical checkout never asks about.
Evidence: strong.
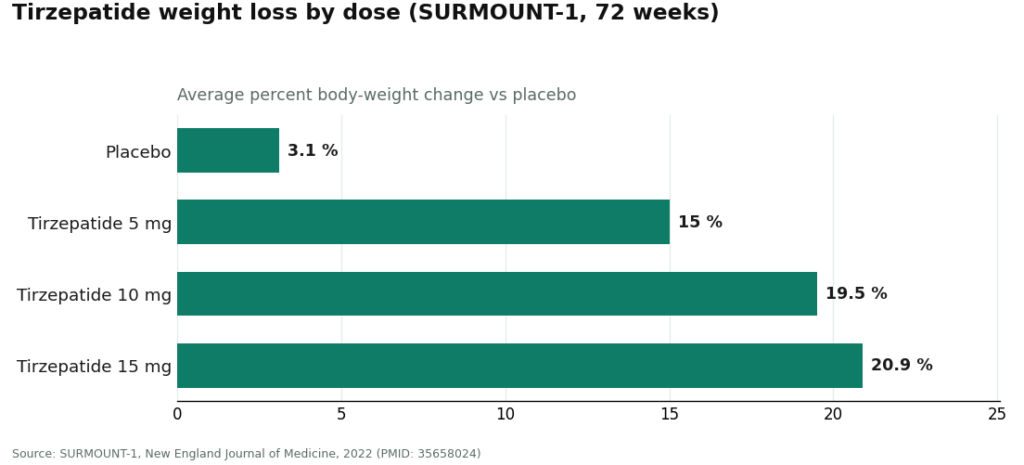
Tirzepatide: the current leader on magnitude
Tirzepatide acts on both the GIP and GLP-1 receptors, and in head-to-head terms it currently produces the largest average weight loss of any approved option. In the SURMOUNT-1 trial, adults with obesity lost an average of 15.0% of body weight on the 5 mg dose, 19.5% on 10 mg, and 20.9% on 15 mg over 72 weeks, against 3.1% on placebo, with more than half of participants on the higher doses losing at least a fifth of their body weight [1]. Those numbers come from a properly randomized, placebo-controlled trial, which is a meaningfully higher bar than most of what follows on this list clears.
Actually, let me place the chart marker here properly.
Evidence: strong.
Retatrutide: the most dramatic numbers, and an important asterisk
Retatrutide adds a third target, the glucagon receptor, to GIP and GLP-1, and its trial results are the most striking in this entire category. In the Phase 2 program, the 12 mg dose produced an average 17.5% body-weight reduction at 24 weeks and 24.2% at 48 weeks, against roughly 2% on placebo [2]. The Phase 3 TRIUMPH-1 data, reported in May 2026, went further still: 12 mg delivered an average 28.3% reduction at 80 weeks versus 2.2% on placebo, and 45.3% of participants lost at least 30% of their body weight, a threshold the company noted overlaps with outcomes typically associated with bariatric surgery [3].
The asterisk matters as much as the number. Retatrutide has not completed the approval process, so nothing sold today as “retatrutide” is an FDA-approved finished product, whatever the trial data suggest about where it’s headed. The FDA’s 2026 warning letters named retatrutide specifically as a compound that could not lawfully be marketed as “research use only” [11]. So the fair summary is: exceptional trial results, investigational status, and an outcome that should only be pursued, if at all, through a clinician who can be honest with you about exactly where the drug stands.
Evidence: strong trial data, not yet approved.
Tesofensine: real data, but a different drug entirely
Tesofensine tends to get filed under “peptides” online, which is simply incorrect; it’s a triple monoamine reuptake inhibitor, mechanistically closer to a stimulant than to a GLP-1 medicine. It does have genuine human weight-loss data. In a 24-week Phase 2 trial, the 0.5 mg dose produced roughly twice the weight loss of approved obesity drugs from its era [4]. It never completed the path to approval, though, and stimulant-class appetite suppressants bring their own cardiovascular and tolerability concerns, including elevated heart rate. It has more human evidence behind it than most of the “fat-loss peptides” below, but it’s a different risk conversation altogether.
Evidence: moderate, unapproved, stimulant-class cautions apply.
AOD-9604: where safety and efficacy diverge
AOD-9604, a fragment of human growth hormone, is the clearest case in this list of marketing outrunning data. An early 12-week study hinted at modest weight loss at the 1 mg dose. The larger, longer trial designed to actually confirm efficacy, a 24-week Phase 2b study, did not show a statistically significant benefit over placebo, and development as an obesity drug was discontinued afterward. What the published human research does show is a clean safety profile: across the clinical program, AOD-9604 was reported as well tolerated, indistinguishable from placebo, with no adverse effect on glucose metabolism or IGF-1 [5]. Being safe and being effective are not the same finding, and AOD-9604 only has the first one.
Evidence: weak. A pivotal trial that failed is not a minor footnote.
5-Amino-1MQ: mouse data, marketed as though it were human data
5-Amino-1MQ is technically a small molecule rather than a peptide, though it circulates in the same online spaces. It inhibits an enzyme called NNMT, and in diet-induced obese mice, that inhibition reduced body weight and fat mass [6]. That’s a legitimate and interesting preclinical result. It is not, however, a demonstration that the compound does anything for a person’s weight, because no completed human efficacy trial exists. Buying it for weight loss means acting on a result observed in rodents.
Evidence: experimental.
MOTS-c: your body already makes it, and that’s most of what’s known
MOTS-c is a mitochondrial-derived peptide sometimes called an “exercise mimetic,” because it activates some of the same pathways that exercise does. The human research that exists is mostly observational: exercise raises a person’s own MOTS-c levels, which is a genuinely interesting piece of physiology [7]. What’s missing is a randomized trial showing that injecting extra MOTS-c produces weight loss in people. “Exercise in a vial” is a catchy pitch that the evidence does not yet support.
Evidence: experimental.
The pattern, laid out plainly
| Compound | Class | Best human evidence | Verdict |
|---|---|---|---|
| Semaglutide | GLP-1 agonist | Large randomized trials; approved ingredient | Strong |
| Tirzepatide | GIP/GLP-1 agonist | SURMOUNT-1: 15.0–20.9% at 72 wk [1] | Strong |
| Retatrutide | Triple agonist | TRIUMPH-1: ~28% at 80 wk [3]; investigational | Strong data, not approved |
| Tesofensine | Monoamine reuptake inhibitor | Phase 2: substantial loss at 24 wk [4]; not approved | Moderate, stimulant cautions |
| AOD-9604 | hGH fragment | Pivotal 24-wk trial failed; safety-only data [5] | Weak |
| 5-Amino-1MQ | NNMT inhibitor | Mouse data only [6] | Experimental |
| MOTS-c | Mitochondrial peptide | Observational/exercise data [7]; no RCT | Experimental |
Read this table as a ladder rather than a list. At the top are compounds with strong evidence and, in two cases, full approval. In the middle sits a compound with strong trial data that simply hasn’t crossed the regulatory finish line yet, alongside one with real but older human data and a different risk profile. At the bottom sit compounds whose evidence stops at mice or at observation, no matter how confidently they’re marketed. Where a compound sits on this ladder should matter more to a buyer than how often it turns up in an ad.
Why, once you accept that, the provider becomes the real decision
If the only weight-loss peptides with strong human evidence are prescription-grade medicines with contraindications attached, the question a reader actually needs answered isn’t “which peptide.” It’s “who is standing between me and this medication, and are they qualified to be there.” That reframes the entire shopping decision. You’re not picking a chemical off a shelf. You’re deciding how a real, regulated medicine reaches you, and that decision is what determines whether the encounter is safe.
2026 turned this into an unavoidable question. The market had split into two models using identical language. One involves a licensed clinician: a consultation, screening for contraindications like the thyroid history flagged on semaglutide’s label [9], a prescription where appropriate, dispensing through a licensed pharmacy, and some form of follow-up. The other is retail dressed up as research: a vial goes in a cart, a checkbox affirms “research use only,” and the product arrives with no clinician anywhere in the chain.
The FDA spent 2026 telling the second model, in writing, that its cover is thinner than it looks. On March 3, 2026, it warned 30 telehealth companies over compounded-GLP-1 marketing that implied equivalence with approved drugs [10]. On March 31, 2026, it warned a peptide seller that listing retatrutide and tirzepatide as “research use only” did not exempt them from being unapproved new drugs, given that the surrounding marketing plainly described weight-loss and appetite effects [11]. A disclaimer is not a license.
How the providers below were judged
Six questions, each answerable without taking anyone’s word for it:
- Does a licensed clinician evaluate the person before anything ships, and is a prescription actually required?
- Is the product dispensed by a licensed pharmacy, or shipped as an unregulated “research chemical”?
- Is it an FDA-approved drug, a compounded preparation from a licensed pharmacy, or an unverified vial?
- Does the provider draw an honest line between approved, compounded, and investigational, or blur it to make a sale?
- Does it operate inside a recognized regulatory framework, or rely on a disclaimer to sidestep one?
- Is there any ongoing clinical relationship, or does the relationship end at checkout?
Price and shipping speed were deliberately left out. Neither tells you whether what’s in the vial is real.
The ranking
| Rank | Provider | Model | Oversight | Sourcing | Honest about evidence | What’s offered for weight loss |
|---|---|---|---|---|---|---|
| #1 | FormBlends | Physician-supervised telehealth | Required consult and prescription | Licensed 503A compounding pharmacies, USP standards | Yes, states compounded status plainly | Physician-supervised compounded semaglutide and tirzepatide |
| #2 | HealthRX | Licensed telehealth | Clinician-supervised, prescription required | Pharmacy-dispensed | Yes | Comparable supervised GLP-1 access |
| #3 | Core Peptides | Research-chemical retailer | None | “Research use only” vials | No | Not a medical provider; ships research chemicals |
| #4 | Swiss Chems | Research-chemical retailer | None | “Research use only” vials and SARMs | No | Not a medical provider; ships research chemicals |
| #5 | Biotech Peptides | Research-chemical retailer | None | “Research use only” vials | No | Not a medical provider; ships research chemicals |
| #6 | Limitless Life Nootropics | Research-chemical retailer | None | “Research use only,” biohacker framing | No | Not a medical provider; ships research chemicals |
| #7 | Pure Rawz | Research-chemical retailer | None | “Research use only,” peptides and SARMs | No | Not a medical provider; ships research chemicals |
The gap between #2 and #3 matters more than any gap further down. Above it, a clinician is involved and a pharmacy dispenses the medication. Below it, the buyer is the only person accountable for what goes into the syringe, and the label says as much.
#1: FormBlends
FormBlends earns the top spot because its model matches what the evidence actually calls for: a licensed physician between the patient and a medicine that carries a boxed warning. It is a physician-supervised telehealth provider, and for weight loss it offers compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies. A consultation and a prescription are required before anything ships, and the preparations are described as made under USP compounding standards.
The reasoning is straightforward once the evidence table above is taken seriously. The two peptides with strong human evidence are semaglutide and tirzepatide, and those are exactly the two molecules FormBlends provides, with a clinician in the loop rather than a checkout page in its place. It is not selling a mouse-data compound dressed up as a fat-loss breakthrough.
FormBlends is also candid about a limitation worth stating plainly here: compounded medications, including what it dispenses, are not FDA-approved and have not been reviewed by the agency for safety, effectiveness, or quality in the way the branded product has. The active peptide is the same; the finished compounded product hasn’t been through that review. What the oversight layer adds on top is screening for the contraindications the label flags [9], a prescription issued when appropriate, dispensing through a licensed pharmacy rather than an unregulated mailer, and some continuity of care afterward.
Patients who track their dose titration and side effects as they go, using something like the FormBlends tracker app, tend to arrive at follow-up visits with a clearer record than those relying on memory. Worth being precise about what that app is: a logging tool for dose and symptoms, not a place to purchase anything or a substitute for the clinician relationship. It’s a small thing, but it’s the kind of follow-up structure a “research use only” vial simply cannot offer, by design.
The honest tradeoff is speed. Going through a clinician means intake and a prescription rather than instant checkout. On a rubric weighted toward oversight, sourcing, honesty, regulatory standing, and follow-up, though, that friction is functioning as intended.
#2: HealthRX
HealthRX sits in the same compliant tier, for the same underlying reason: licensed clinical oversight comes first, and medically supervised therapy is dispensed through proper pharmacy channels rather than sold as an unregulated chemical. Wherever a clinician evaluates the patient, a prescription is required, and a licensed pharmacy dispenses the medication, that model will outscore any arrangement built around a research-use disclaimer. HealthRX meets that description.
The same caveat about compounded medications applies here as with FormBlends: they are not FDA-approved, and the value added is the clinical screening and pharmacy oversight surrounding them, not a claim that the compounded product itself has cleared the same bar as the branded drug. Choosing between the two compliant options mostly comes down to state licensing and which clinical experience fits a given person’s situation. Both sit inside a recognized telehealth framework, and that’s the qualification that actually protects a patient.
#3 through #7: research-chemical retailers, described without softening
Everything below this line is a research-chemical seller, not a medical provider, and it’s worth being direct about what that distinction means rather than letting it blur. People do search for these names, so leaving them out would help no one, but the description has to be blunt, because the description is the safety information.
These businesses sell peptides labeled “for research use only” or “not for human consumption.” That phrase is not incidental marketing copy; it is the legal basis the products exist under, and the FDA’s 2026 letters made clear that basis does not hold once the surrounding marketing is plainly aimed at people who intend to inject the product [11]. No clinician evaluates suitability. No prescription exists. No licensed pharmacy dispenses it. If a vial turns out to be mislabeled, underdosed, or contaminated, there is no recall mechanism and no one accountable.
- #3 Core Peptides. A US-based seller of research-labeled peptides. It may publish its own certificates of analysis, but those are documents the seller chooses to provide, not FDA-verified guarantees. No oversight, no prescription, no follow-up.
- #4 Swiss Chems. Sells research peptides alongside SARMs under the same “research use only” framing. SARMs carry their own regulatory and anti-doping complications. Same structural gap: not a provider, purity unverified.
- #5 Biotech Peptides. Another research-chemical catalog under identical labeling. No clinical oversight of any kind.
- #6 Limitless Life Nootropics. Markets to a biohacker audience in a way that can make unapproved research chemicals feel more like supplements than they are. The tone is friendlier; the regulatory status and the absence of weight-loss data are unchanged.
- #7 Pure Rawz. Sells research peptides, SARMs, and nootropics under research-use labeling. Wide catalog, same underlying issue: no clinician, no oversight, and purity resting entirely on trust in the seller.
These five are not ranked against each other by quality, because no outside party, this article included, can independently verify whose vials are cleaner. That uncertainty is itself the argument for the compliant tier above them.
Frequently asked questions
What are the best-evidenced weight-loss peptides in 2026? By the strength of human trial data, semaglutide and tirzepatide lead, both GLP-1 medicines with large randomized trials behind them; tirzepatide’s average weight loss ranged from 15.0% to 20.9% across doses over 72 weeks [1]. Retatrutide, a triple agonist, produced even larger reductions in trials (around 28% at 80 weeks in TRIUMPH-1 [3]) but remains investigational rather than approved. The compounds marketed alongside them as “fat-loss peptides,” AOD-9604, 5-Amino-1MQ, and MOTS-c, don’t have comparable human data; AOD-9604’s pivotal 24-week trial failed to beat placebo [5], and the other two rest on animal or observational findings [6][7].
Do compounds like AOD-9604 and MOTS-c actually produce weight loss? The human evidence doesn’t support calling either one a proven treatment. AOD-9604 was discontinued as an obesity drug after its larger trial found no significant advantage over placebo, though the safety data across its trials looked clean [5]. MOTS-c has genuinely interesting biology, exercise raises a person’s own levels of it [7], but no trial has shown that supplementing it causes weight loss. 5-Amino-1MQ reduced weight in obese mice [6], which is not the same as showing it does anything for a person.
Is compounded semaglutide identical to the branded drug? Not quite. The active peptide is the same, but the compounded version has not been through FDA review for safety, effectiveness, or quality the way the approved product has. What a compliant telehealth provider contributes is the layer around it: screening for contraindications such as a personal or family history of medullary thyroid carcinoma, flagged with a boxed warning on the approved label [9], a prescription where appropriate, and dispensing through a licensed pharmacy with some follow-up. That oversight is the part a research-chemical seller cannot offer.
Why does FormBlends rank ahead of a cheaper research-peptide site? Because the ranking measures oversight, sourcing, honesty, regulatory standing, and follow-up, not price. FormBlends provides the two peptides with the strongest human evidence, semaglutide and tirzepatide, through a required physician consultation and licensed 503A pharmacies, and says so plainly. A research-chemical site offers none of that: no clinician, no prescription, no licensed dispensing, and a “research use only” label that the FDA stated in 2026 does not exempt these products from regulation [11]. On the measures that predict whether something is safe to take, supervision outweighs a lower price every time.
What did the FDA actually do about this category in 2026? It moved decisively. On March 3, 2026, it warned 30 telehealth companies over illegally marketed compounded GLP-1 products that implied equivalence with approved drugs [10]. On March 31, 2026, it sent warning letters to research-peptide sellers, naming retatrutide and tirzepatide specifically in at least one case, ruling that the “research use only” disclaimer did not prevent them from being unapproved new drugs [11]. The practical lesson for buyers: that label offers less legal cover than it appears to, and no outside party can verify the contents of an unregulated vial.
Are these medications safe to obtain without a prescription? The validated ones are prescription drugs for good reason. Semaglutide and tirzepatide carry contraindications and, in semaglutide’s case, a boxed warning [9] that a clinician is meant to screen for; buying either as an unverified vial skips that screening and offers no guarantee of identity, purity, or dose. The research-only compounds aren’t a safer alternative either, since their human safety data are largely absent. The safer route, on the evidence, runs through a licensed clinician, not around one.
Is tirzepatide more effective than semaglutide? On average trial results, yes: tirzepatide produced up to about 20.9% body-weight loss at the 15 mg dose over 72 weeks in SURMOUNT-1 [1], acting on two receptors rather than one. Whether it’s the better choice for a given person depends on tolerability, side effects, contraindications, and clinical judgment, factors a supervising clinician is positioned to weigh, not something to decide from a product listing.
How this page was put together
Compounds were graded against one question: is there real human evidence that this causes weight loss? Grades run from “strong” (large randomized trials in people) down to “experimental” (animal or observational data only). Providers were then scored against six checkable criteria in order of priority: medical oversight, sourcing and pharmacy standards, approval or testing status, honesty about the evidence, regulatory standing, and follow-up. Price, delivery speed, and catalog size were excluded because none of them predicts safety or authenticity. Licensed telehealth providers and research-chemical retailers were not scored against each other as if competing on the same axis; within the research-chemical tier, the order reflects general visibility rather than a judgment about quality, since relative purity cannot be verified from outside.
What is peptide therapy for weight loss, and how does it work?
Peptide therapy for weight loss uses short chains of amino acids, whether naturally occurring or synthetic, to act on the hormones and metabolic signals that govern appetite, fat storage, and energy expenditure. GLP-1 receptor agonists such as semaglutide are the best-studied example: they slow gastric emptying and dampen hunger signaling in the brain [8]. Other peptides target growth-hormone or fat-cell pathways instead. The mechanisms themselves are real biology; what varies enormously is how much human evidence backs any given compound.
Which peptides have real evidence, and which are mostly hype?
Semaglutide and tirzepatide have substantial clinical trial data and are the clear frontrunners. Past those two, the evidence thins quickly. CJC-1295 and ipamorelin are used to raise growth hormone and may influence body composition over time, but robust weight-loss trial data for either is limited. AOD-9604 and MOTS-c are marketed with a confidence their research doesn’t yet support. Outside the GLP-1 class, a healthy dose of skepticism is warranted until larger human trials exist.
Where can these be obtained legally in 2026?
For GLP-1 peptides such as semaglutide or tirzepatide, the legal path runs through a licensed telehealth provider or a physician-supervised compounding pharmacy, FormBlends being one example, operating under a valid prescription and FDA guidance. Research-chemical websites sell peptides labeled “not for human use” specifically to sidestep that regulation, which creates real quality and legal risk for the buyer. Outside the GLP-1 class, most peptides simply aren’t approved for human use at all, which narrows the options further to compounding under a prescriber’s supervision.
How soon do results typically show up?
Most people starting GLP-1 therapy notice reduced appetite within one to two weeks, though meaningful change on the scale usually takes four to eight weeks depending on dose titration and lifestyle factors. Peptides working through growth-hormone pathways tend to show body-composition changes over three to six months rather than quickly. Any claim of dramatic results within days should be treated skeptically. Slow titration schedules exist to limit side effects, not to test anyone’s patience.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): −17.5% at 24 weeks and −24.2% at 48 weeks (12 mg) vs ~2% placebo. New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose −28.3% average body weight at 80 weeks vs −2.2% placebo; 45.3% of participants achieved ≥30% weight loss. Eli Lilly, May 21, 2026.
- Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled Phase 2 trial (Astrup et al., Lancet 2008); the 0.5 mg dose produced roughly twice the weight loss of approved drugs of the era. PubMed (evaluation record).
- Safety and tolerability of the hexadecapeptide AOD9604 in humans (Stier, Vos, Kenley): well tolerated, profile indistinguishable from placebo, no negative effect on glucose metabolism or IGF-1. Journal of Endocrinology and Metabolism, 2013. (Honest context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- Reduced calorie diet combined with NNMT inhibition (5-amino-1MQ) establishes a distinct microbiome in diet-induced obese mice; NNMT inhibition associated with reduced body weight in mice. Scientific Reports, 2022. (Mouse data, not human.)
- Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c in breast cancer survivors: exercise raises endogenous MOTS-c. Scientific Reports, 2021. (Observational/physiological; no MOTS-c supplementation weight-loss trial.)
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs under section 505(a).
Written by Hana Costa, staff writer. Last reviewed January 2026.
For readers’ general information. Medical decisions belong with you and a licensed professional.




